TL; DR - Key takeaways
- Alerts are not the answer. Clinical Provider Order Entry (CPOE) alert override rates run between 46.2% and 96.2%. More notifications make care worse, not safer.
- Personalised CDSS is bidirectional. It ingests live signals from EHRs, devices, labs, and patient-reported data; advances the care pathway automatically; and verifies that each task is completed.
- Interconnected and robust architecture: pathway intelligence, workflow triggering, clinical action support, closed-loop follow-through, governance and analytics, and a patient wellness layer covering nudges, personalised tests, and prior authorisation, fronted by a conversational interface.
- Personalisation is the core. Tailoring care to comorbidities, lifestyle, and social determinants to ensure healthier lifestyle for patients
-
Governance is the unlock for trust at scale. Versioned pathways, audited overrides, and surfaced variation turn a clinical pilot into managed infrastructure.
Why traditional clinical decision support is failing
Traditional clinical decision support fails because it was designed for a world of paper charts and discrete orders, not a continuous, multi-source data environment. It relies on static rules and pop-ups that interrupt, rather than orchestrate, care. The data is unambiguous: a systematic review of computerised provider order entry behaviour reported alert override rates between 46.2% and 96.2% across studied environments, meaning clinicians routinely ignore even high-severity prompts.
The cost is twofold. Clinicians spend roughly two hours on EHR and desk work for every hour of direct patient care, plus another one to two hours of after-hours “pajama time” each night. Patients, meanwhile, get reactive medicine: subtle signs of deterioration sit un-synthesised in the chart until someone happens to look. Digital adoption is at an all-time high, yet the cognitive load on frontline clinicians has never been heavier. The path forward is not more notifications. It is a Personalised CDSS that spans triage, decision support, escalation, prior authorisation, and closed-loop follow-up.
What is a Personalised CDSS?
A Personalised Clinical Decision Support System (Personalised CDSS) is an AI-driven, longitudinal layer that ingests live signals from EHRs, devices, labs, and patient-reported inputs; matches each individual’s state to evidence-based pathways tailored to their comorbidities, social determinants, and preferences; triggers the right persona at the right moment; automates administrative friction such as prior authorisation; and verifies completion of every task in a closed loop.
Where traditional CDS sits beside the workflow and asks the clinician to act on each prompt, a Personalised CDSS sits inside the workflow and advances the care state automatically, retaining the clinician for judgement, sign-off, and exceptions. It is built on four operating principles.
- Personalised: Care is tailored to the individual context: comorbidities, lifestyle, social determinants, and patient preferences, not just the disease code.
- Predictive: Longitudinal data drives proactive risk management, replacing reactive treatment of complications with early intervention.
- Integrated: Insights are embedded natively within the EHR and clinician workflow, ensuring zero-friction adoption.
- Actionable: The distance between insight and intervention collapses through one-click order sets, auto-drafted prior authorisations, and personalised patient nudges.
Traditional CDS vs Personalised CDSS
The clearest way to see the shift is to compare the two operating models directly across the dimensions that matter to clinical, operational, and quality leaders.
|
Dimension |
Traditional CDS |
Personalised CDSS |
|
Trigger model |
Rule-based pop-ups, fired on order entry |
Continuous matching of live, longitudinal signals against versioned, individualised pathways |
|
Patient context |
Limited to fields visible at the moment of the alert |
Co-morbidities, SDOH, vitals, labs, devices, intake, and prior pathway progress |
|
Personalisation |
One-size-fits-all rule logic |
Patient-specific dosing, risk scoring, nudges, and test selection |
|
Administrative work |
Clinician-driven prior authorisation, manual referrals |
AI-drafted prior authorisation, automated documentation, scheduled follow-ups |
|
Patient engagement |
Episodic, paper-based education |
Personalised digital nudges, wellness tracking, and self-management coaching |
|
Follow-through |
Ends when the clinician dismisses the alert |
Tracks tasks to verified completion with auto-escalation when checkpoints are missed |
|
Governance |
Static rule library, opaque override behaviour |
Versioned pathways, logged overrides, and surfaced variation by service line |
|
Measurability |
Override rate, with limited outcome attribution |
Time-to-bundle, adoption telemetry, A1C deltas, ED-visit reduction, and PMPY savings |
What does a Personalised CDSS entail?
A Personalised CDSS replaces static alerts with adaptive, auditable, individualised guidance that automates care pathways, prior authorisation, wellness monitoring, and personalised testing. Six capabilities, fronted by a conversational interface, define the architecture.
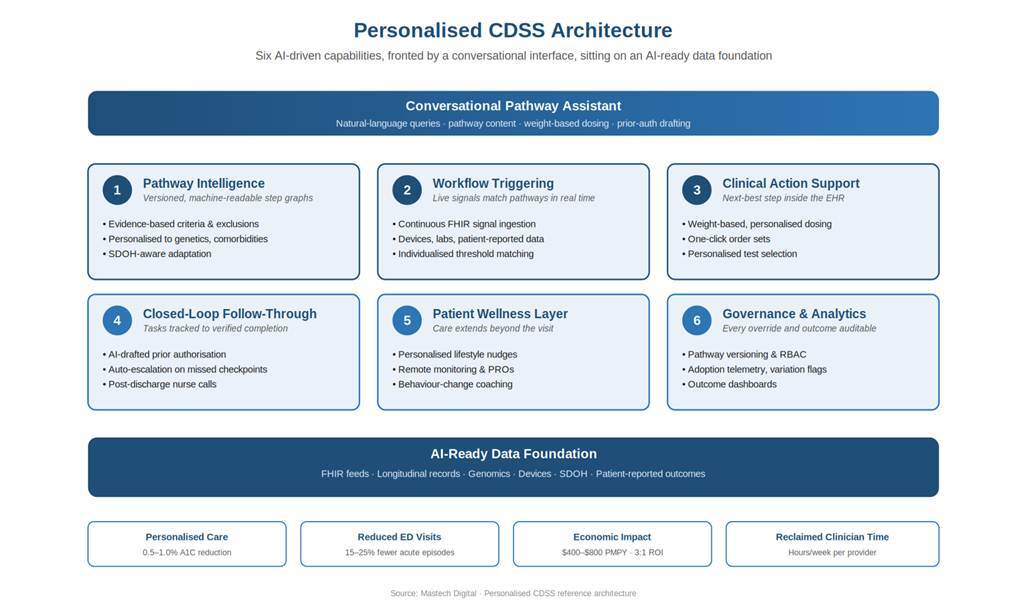
Figure 1: Six AI-driven capabilities sit on an AI-ready data foundation and surface to clinicians through a conversational pathway assistant with illustrative impact values
|
1. Pathway intelligence Static protocols become versioned, machine-readable step graphs. Evidence-based pathways are ingested with criteria, exclusions, evidence links, and version control, then personalised against patient genetics, comorbidities, and social context. |
2. Workflow triggering Live signals match personalised pathway criteria in real time. Vitals, labs, device data, and patient-reported inputs are continuously compared against individualised thresholds to launch the right protocol at the right moment. |
|
3. Clinical action support The next-best step surfaces inside the EHR. Weight-based dosing, evidence citations, personalised test recommendations, and one-click order sets keep the clinician in flow rather than chasing references. |
4. Closed-loop follow-through Tasks are tracked to verified completion. AI-drafted prior authorisations, post-discharge nurse calls, personalised patient nudges, and escalation paths run on auto-pilot when checkpoints are missed. |
|
5. Patient wellness layer Care extends beyond the visit. Personalised lifestyle nudges, remote monitoring, behaviour-change coaching, and SDOH-aware outreach keep patients engaged between encounters. |
6. Governance and analytics Every pathway, override, and outcome is auditable. Versioning, adoption telemetry, variation flags, RBAC, and audit trails make the system measurable and trustworthy. |
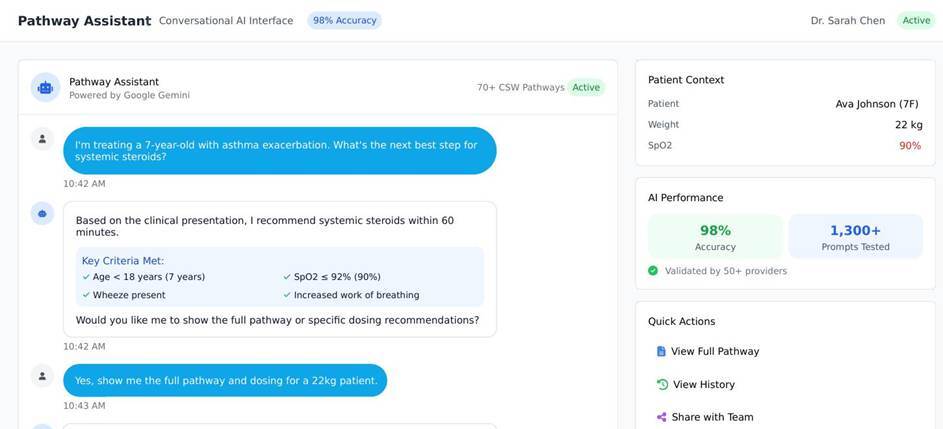
Conversational pathway assistant
A natural-language interface sits across all six layers. Plain-language queries (“What’s the next-best step for systemic steroids?”, “Show me dosing for a 22 kg patient” etc.) return pathway content, dosing tables, flowcharts, and pre-filled administrative artefacts, grounded in the same evidence-versioned pathway content the engine uses for automated actions.
POINT OF VIEW: The unlock is the step graph, not the model
Across the deployments we have led, the highest-leverage step is rarely the model. It is the step graph. Most health systems already have evidence-based pathways. What they don’t have is those pathways encoded as machine-readable state, wired to live FHIR feeds, personalised against patient-level data, and instrumented for variation. That foundational data engineering is where the Personalised CDSS unlock comes from. The conversational layer is what clinicians notice; the step graph and AI-ready data foundation are what make it work.
How a Personalised CDSS automates care pathways, prior authorisation, and patient wellness
Personalisation alone is not enough. The economics only work when administrative drag is removed and patient engagement is sustained between visits. A modern Personalised CDSS automates four pressure points that traditional CDS leaves untouched.
Automated care pathway execution
Care pathways are no longer PDFs printed for the unit binder. Each pathway is a versioned step graph with explicit entry criteria, time targets, branching logic, and completion checkpoints. The Personalised CDSS matches the patient against the pathway in real time, updates state when criteria are met, and routes exceptions to the right clinician. Time-to-bundle, adoption by service line, and provider-level adherence become managed metrics rather than annual board slides.
Prior authorisation automation
Prior authorisation is one of the largest sources of administrative burden in U.S. healthcare. A Personalised CDSS reads the proposed order, pulls the patient’s clinical justification from the longitudinal record, drafts the payer-specific prior-authorisation packet, and routes it for clinician sign-off through payer APIs. The clinician reviews and signs; the system handles the paperwork, status tracking, and appeals.
Personalised patient nudges
Generic reminders are ignored at rates similar to clinical alerts. Personalised nudges are different: they are timed, channel-matched, language-matched, and tuned to the individual’s health literacy, motivation profile, and prior response. A patient who responds to data sees a glucose trend; a patient who responds to social proof sees how peers are doing; a patient who has missed three medication doses gets a phone call from the care team.
Personalised tests and screening
Screening guidelines are population-level by design. A Personalised CDSS overlays the individual: family history, prior results, comorbid conditions, and adherence patterns. The result is a personalised testing cadence that orders the right test, at the right interval, with the right pre-test counselling, and routes results back into the pathway for action.
Wellness and between-visit care
The closed loop extends past the encounter. Remote monitoring data, patient-reported outcomes, and behavioural signals stream into the same pathway engine. Deterioration is caught early; sustained progress is reinforced; social-determinant barriers (transportation, food security, caregiver availability) trigger care-team outreach rather than silent disengagement.
Diabetes case study: meet Maria
Diabetes is the right place to start. The need is urgent, and the data is rich. More than 30 million Americans live with diabetes, and the cost to the country has climbed from $327 billion to over $413 billion a year. Maria, a 56-year-old with Type 2 Diabetes, shows what the technology actually does for one person.
Maria’s situation
- Her blood sugar is too high, and her kidneys have started to weaken.
- She is on three medicines, including one that can cause low-blood-sugar episodes.
- She lives alone, has trouble getting to appointments, and prefers messages in Spanish.
What the Personalised CDSS does for her
The system reads everything in Maria’s record together and spots a problem her care team would otherwise have to piece together. The system shows that there are newer drug classes that would lower her sugar, protect her kidneys, and help with her weight at the same time. The system suggests the swap right inside the doctor’s screen, with the evidence behind it.
The system also drafts the insurance paperwork for the new medicine. It sets up a check-in two weeks out, to see how her sugar is responding. It orders the kidney test that should go with this kind of change. And because her record flagged that she struggles to get to appointments, it books her follow-up with transport help arranged. The doctor reviews and signs.
Figure 2: Maria’s care journey, before and after. What used to take 15 minutes of chart-digging happens in under 30 seconds, and the follow-up runs itself.
Paediatric scenario: meet Mia
Diabetes shows the slow build of better care over months. Mia, age 4, shows what happens in minutes when a child is seriously ill. At 2 in the afternoon her mother types her symptoms into the hospital app: high fever, very tired, hardly drinking. In most hospitals, this would mean a phone call, a wait, and a lot of paper. Here, the system reads the symptoms, spots the warning signs, and starts moving.
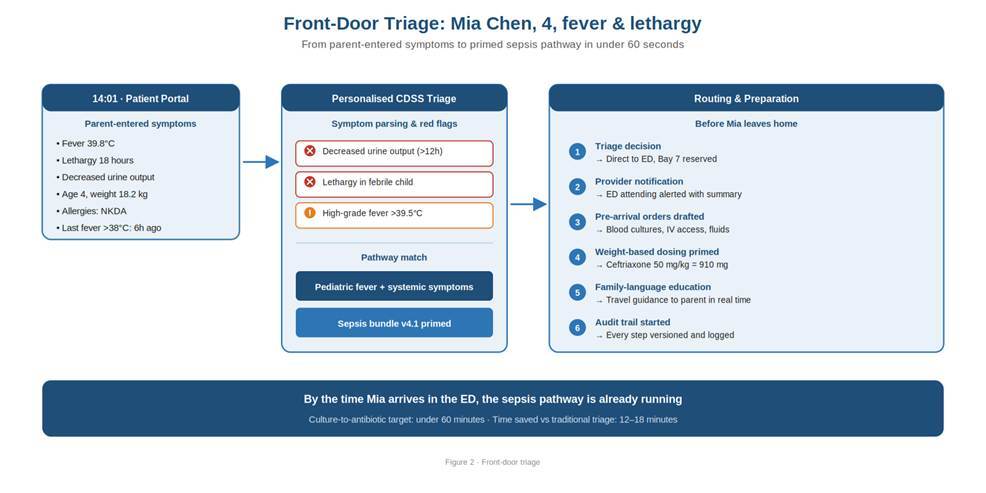
Figure 3. The front door, before Mia leaves home. The system reads her symptoms, picks the right care plan, and tells the ED to expect her.
By the time Mia arrives, the room is ready and the right tests and medicines are already drawn up at the right doses for her size. The doctor sees one screen with three things to do, in order, with the timing each one needs. She reviews and approves. The system handles the prep work.
Figure 4. (Illustrative) One screen, three clear next steps. The doses are already calculated for Mia’s weight; the doctor reviews and signs.
The system keeps watching
A good suggestion at the start isn’t enough. Mia’s condition can change quickly, so the system keeps checking. If her heart rate stays high after the first round of treatment, it pulls in the intensive care team automatically. If a key blood test crosses a danger line, the more serious treatment plan kicks in. Nothing waits for someone to notice.
Figure 5. The system keeps watching. If Mia gets worse instead of better, the right specialists are pulled in without anyone having to remember to call.
Going home is part of the plan
When Mia is well enough to go home, the visit notes are drafted along with the nurse follow-up call and the next doctor’s visit already on the calendar. If they miss a check-in, the care team knows. The same loop that handled the emergency handles the recovery.
Figure 6. The visit doesn’t end at the door. Notes, instructions, and follow-up are all queued up before the family leaves.
Governance is the unlock for trust at scale
Health system leaders have heard “AI in the clinic” promises before. What turns a pilot into infrastructure is the governance layer. Every pathway is versioned. Every override is logged. Variation is surfaced.
Median time-to-antibiotics, adoption by service line, provider-level adherence, prior-authorisation turnaround, and personalised-nudge response rates all become managed metrics. The discipline mirrors what we have argued elsewhere about trusted data foundations in healthcare: AI without governance is not AI; it is risk dressed up as innovation.
Figure 7. Governance and analytics. Pathway adoption, variation flags, and version history are made visible to clinical, quality, and informatics leaders.
The platform extensibility to all therapy areas
The Personalised CDSS architecture is designed as a scalable platform. The same set of capabilities apply directly to heart failure, COPD, hypertension, oncology continuity of care, and post-surgical recovery. By solving for the complexity of diabetes: personalisation, prior authorisation, between-visit wellness, and SDOH-aware follow-up, health systems build the foundation for total chronic care management.
What to do next
For health system CIOs, CMIOs, payers, and quality leaders evaluating where to invest in the next AI cycle, the pragmatic starting points are sequential and measurable.
- Audit one high-acuity, high-volume pathway end-to-end and quantify where time, money, and outcomes are actually lost.
- Move that pathway from PDF to a versioned, machine-readable step graph wired to live EHR signals, with personalisation layered on top.
- Deploy a Personalised CDSS for one cohort with closed-loop follow-through, prior-authorisation automation, and personalised nudges, instrumented so adoption, variation, and outcomes are visible from day one.
- Establish governance early: versioning, override logging, RBAC, and outcome dashboards so the pilot scales as managed infrastructure, not an experiment.
The organisations that win the next decade of clinical AI will not be the ones with the loudest alerts. They will be the ones whose Personalised CDSS quietly, reliably does the right thing for each patient, and proves it.
References
- Bryant AD, Fletcher GS, Payne TH. Drug–drug interaction alert override and appropriateness: a systematic review. JMIR Medical Informatics / Journal of the American Medical Informatics Association. Reported alert override rates between 46.2% and 96.2% across CPOE systems.
- Sinsky C, Colligan L, Li L, et al. Allocation of physician time in ambulatory practice: a time-and-motion study. Annals of Internal Medicine, 2016. Physicians spend approximately two hours on EHR and desk work for every hour of direct patient care.
- Schlapbach LJ, Weiss SL, Bembea MM, et al. Delays to antibiotics in the emergency department and risk of mortality in children with sepsis. JAMA Network Open, 2024. Multicentre cohort of 19,515 pediatric patients across 51 U.S. children’s hospitals; antibiotic delay beyond 330 minutes was associated with increased sepsis-attributable mortality.
- U.S. Centers for Disease Control and Prevention. QuickStats: hours per day documenting clinical care outside normal office hours, 2019. MMWR, 2021. 91% of office-based physicians reported after-hours documentation.
- American Medical Association. EHR time across specialties: a five-year analysis of more than 200,000 physicians. Journal of General Internal Medicine, 2024.
- JMIR Medical Informatics, 2020. Machine-learning approach to reduce alert fatigue (citing 90% override rates).
- Medical Economics, 2022. Physicians spend 4.5 hours a day on electronic health records.
- American Diabetes Association, 2024. Economic costs of diabetes in the U.S. ($327B historical context).
Annals of Family Medicine, 2017. Tethered to the EHR: primary care physician workload assessment.
Frequently asked questions
A Personalised Clinical Decision Support System is an AI-driven, longitudinal layer that ingests live data from EHRs, devices, labs, and patient-reported inputs, matches each individual’s state to evidence-based pathways tailored to their genetics, comorbidities, and social determinants, automates administrative steps such as prior authorisation, delivers personalised nudges and tests, and verifies completion of every task in a closed loop.
Traditional CDS issues rule-based pop-ups at the moment of order entry and ends when the clinician dismisses the alert. A Personalised CDSS continuously matches longitudinal patient data against versioned pathways, automates care-pathway execution and prior authorisation, sends personalised patient nudges, and tracks every task to verified completion.
An AI-ready data foundation (live FHIR feeds and longitudinal patient records), evidence-based pathways encoded as versioned, machine-readable step graphs, native EHR integration, robust governance (versioning, RBAC, audit trails, override logging), and a personalisation layer that incorporates genetics, comorbidities, and social determinants.
