
Executive snapshot
The U.S. healthcare workforce is extremely burdened on time. Every additional hour clinicians spend on admin tasks is an hour subtracted from patient care, supervision, teaching, and recovery. Hiring alone cannot close that gap. The path forward is to redesign the work itself, using ambient intelligence, predictive analytics, and embedded automation to lift the administrative load off the clinician and put cognition back where it belongs: with the patient.
Key takeaways
- Why workforce supply alone cannot fix the current shortage, and what the verifiable evidence shows.
- How documentation burden, quantified in peer-reviewed research, translates directly into burnout, attrition, and patient safety risk.
- A “Nurse-in-the-Loop” operating model that augments clinical judgment instead of attempting to replace it.
- How Mastech Digital sequences ambient AI, predictive workforce intelligence, and process automation into a single capacity-optimization program.
The shortage is structural, not cyclical
Workforce data from the 2024 National Nursing Workforce Study, conducted by the National Council of State Boards of Nursing (NCSBN), describes a system that is recovering on the surface and eroding underneath. More than 138,000 nurses have exited the workforce since 2022, and roughly 40 percent of the surveyed registered nurses indicated an intent to leave the workforce or retire within the next five years. Stress, burnout, workload, understaffing, and inadequate compensation lead the cited reasons. Each of them is a workflow problem before it becomes a hiring problem.
 Figure 1. The healthcare workforce crisis at a glance
Figure 1. The healthcare workforce crisis at a glance
Where the clinical hour actually goes
The most under-discussed driver of attrition is the quiet redirection of clinical time into data entry. Peer-reviewed observational research has shown that nurses document between 600 and 800 manual data points per 12-hour shift, equivalent to roughly one entry every 1.11 minutes (Moy et al., Applied Clinical Informatics, 2022; Collins et al., JAMIA, 2019). Other observational studies place EHR-documentation time at 19 to 40 percent of a 12-hour shift, depending on unit and acuity.

Figure 2. The documentation burden
Translate that into a workflow picture. A clinician's attention is being interrupted, on average, more than once per minute by the act of recording, not interpreting, clinical reality. This is a cognitive-load problem with measurable downstream effects on emotional exhaustion, perceived control, and intent to stay.
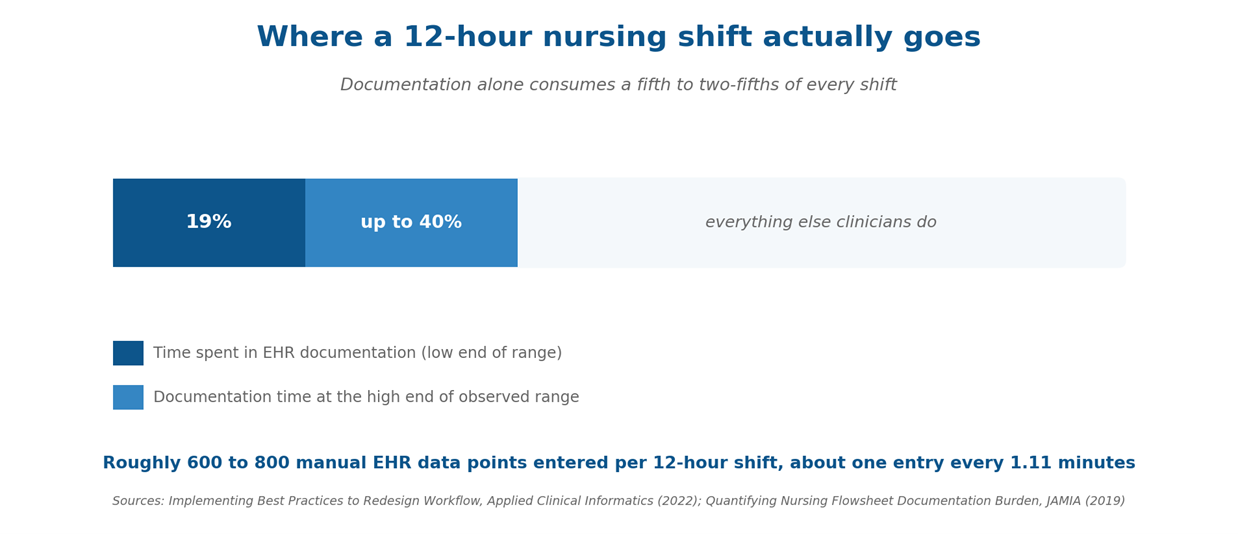
Figure 3. A meaningful slice of every shift is consumed by structured data entry, not direct care.
From documentation burden to patient risk
The link between staffing load and patient outcomes is one of the most replicated findings in health services research. The landmark Aiken et al. analysis (JAMA, 2002) showed that each additional patient in a nurse's average workload was associated with a 7 percent increase in the likelihood of inpatient mortality and failure-to-rescue. When administrative work pushes a nurse's effective span of attention beyond what the staffing ratio would suggest, the safety effect is functionally identical to understaffing, even when the headcount on the floor looks correct.
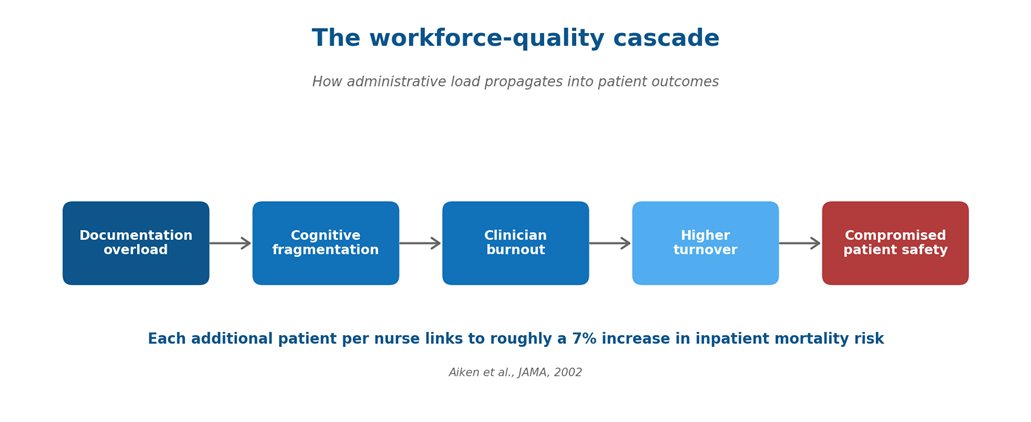
Figure 4. Documentation overload propagates through cognition, retention, and ultimately patient outcomes.
Why hiring more will not solve this
The instinctive response to a workforce gap is to recruit harder. The math no longer supports that as a standalone strategy. Recruitment timelines for experienced RNs averaged 83 days in the 2025 NSI report, vacancy rates remain elevated, and a sizeable share of new hires leave within their first year. Pouring more clinicians into an unchanged workflow simply distributes the same documentation burden across slightly more shoulders, and the people most likely to leave are the ones the burden affects most.
Our point of view: structured flowsheet documentation, as it exists today, will not survive the decade. Within five years, the leading provider organizations will treat manual EHR entry as a fallback rather than the default, with ambient capture handling the overwhelming majority of routine clinical documentation. Health systems that wait for that shift to be proven before adopting it will spend the intervening years subsidizing avoidable burnout, and losing the clinicians most willing to teach a new way of working.
Capacity must be created, not just hired. That means reclaiming clinician minutes from the EHR, the inbox, and the handoff, and reinvesting those minutes in care delivery, mentorship, and recovery. This is the central design principle behind AI-embedded workforce enablement.
Vision 2026: an AI-embedded workforce
The next generation of clinical workflow assumes that the keyboard is not where care happens. Three categories of AI capability are already being deployed at scale, and each addresses a distinct dimension of the capacity problem.
Figure 5. The three capability pillars that compound capacity when sequenced together.
Ambient documentation is the practice of letting AI passively capture a clinical encounter and produce a structured draft note in the EHR, which the clinician then reviews and signs. Ambient AI listens to the clinical encounter, the conversation, the context, and the structured signals from connected devices, and produces a draft note mapped to the relevant EHR fields. The clinician reviews, edits, and signs. The keyboard becomes the exception, not the default.
Predictive workforce intelligence is the application of forecasting models to staffing decisions, combining historical census, patient acuity, scheduled procedures, and external signals to anticipate shift-level demand. Forecasting models combine historical census, acuity, scheduled procedures, and external signals (seasonality, local epidemiology, even weather) to predict shift-level demand. Staffing managers can pre-position float pool, flex cross-trained teams, and reduce reactive agency spend, the single most volatile line item on most operating budgets.
Embedded process automation is the targeted automation of repetitive structured tasks (prior authorization, intake, coding assistance, follow-up scheduling) so clinical and operational teams retain only the judgment-heavy decisions. Prior authorization, intake, coding assistance, discharge instructions, follow-up scheduling. These are the connective tasks that quietly accumulate across the day. Targeted automation removes the repetitive structured work, so clinicians and ops teams retain only the judgment-heavy decisions.
The Nurse-in-the-Loop principle
AI in clinical settings should augment expertise, not arbitrate it. The Nurse-in-the-Loop model is an operating model where AI handles capture, synthesis, and drafting. The clinician retains review, contextualization, and final accountability. Every output is editable. Every decision is auditable. Every model is monitored for drift.
This matters for three reasons. First, clinical judgment depends on nuance that a model cannot fully see: the patient's tone, a family member's worry, an off-pathway symptom. Second, regulatory and liability frameworks rest on the principle of clinician oversight. Third, trust is itself an adoption variable. Tools that ask clinicians to surrender judgment will not be used. Tools that give clinicians their time back will become indispensable.
Figure 6. The Nurse-in-the-Loop workflow keeps clinical judgment central while moving capture and synthesis to AI.
How Mastech Digital operationalizes capacity optimization
Workforce enablement is a sequenced program, clinical, technical, and organizational, that stages value before it scales. The model we deploy with provider organizations follows four moves.
Figure 7. The four-move operating model: diagnose, sequence, govern, measure.
Diagnose the time leakage
Before introducing AI, we instrument the work. EHR audit logs, vendor telemetry, time-and-motion observation, and direct clinician interviews are combined into a quantified map of where clinical hours are actually going. This becomes the baseline against which every later intervention is measured.
Sequence the interventions
Ambient documentation, predictive scheduling, and process automation are sequenced based on which workflow drains the most hours per role, and which integration paths are cleanest in the existing EHR and identity stack. The first intervention is chosen for ROI velocity, not for technical novelty.
Govern the models
Every deployed model is wrapped in a governance layer: documented training data lineage, bias and accuracy monitoring, role-based access, and clinician feedback channels that flow back into evaluation. Health sciences AI without governance is a liability, and an adoption killer.
Measure what matters
Capacity programs should be evaluated on clinician time returned, EHR after-hours work reduced, agency and overtime expense displaced, voluntary turnover trend, and patient-facing quality indicators, in that order. Throughput metrics that ignore the clinician experience tend to recreate the burnout problem they were meant to solve.
Across our health-sciences engagements, the pattern is consistent: when capacity programs are diagnosed before they are deployed, the first wave of ambient documentation typically lands in a step-down setting, because the per-encounter time saved compounds fastest there. The tighter the integration with the existing EHR and identity stack, the faster clinicians stop treating the tool as an experiment and start treating it as the default.
What good looks like
A health system that has done this well does not feel different in dramatic ways. The schedule still has gaps. The pager still goes off. What changes is the quality of the hour: fewer keyboard interruptions, fewer after-shift charting marathons, fewer reactive scrambles for coverage. Documentation closes near the bedside instead of from the parking lot. Schedulers act on a forecast rather than reacting to a vacancy. New nurses, the cohort most likely to leave in the first year, see a workplace that respects their time.
The strategic result is the same outcome, achieved differently: more capacity, lower cost-per-encounter, and a workforce that has reasons to stay. The path to that result is a workflow redesigned around the clinician, with AI embedded in the process.
Sources
- National Council of State Boards of Nursing. 2024 National Nursing Workforce Study. NCSBN, 2025.
- NSI Nursing Solutions, Inc. 2025 NSI National Health Care Retention and RN Staffing Report.
- Aiken LH, Clarke SP, Sloane DM, Sochalski J, Silber JH. Hospital Nurse Staffing and Patient Mortality, Nurse Burnout, and Job Dissatisfaction. JAMA. 2002;288(16):1987 to 1993.
- Moy AJ et al. Documentation Burden in Nursing and Its Role in Clinician Burnout Syndrome. Applied Clinical Informatics, 2022.
- Collins SA et al. Quantifying and Visualizing Nursing Flowsheet Documentation Burden in Acute and Critical Care. JAMIA, 2019.
Frequently Asked Questions
AI-embedded workforce enablement is the integration of ambient documentation, predictive workforce intelligence, and process automation directly into clinical workflows, with the goal of returning clinician time to patient care rather than to administrative tasks. It is distinct from generic “AI in healthcare” because it is workflow-first: the technology is selected and sequenced based on where clinical hours are actually being lost.
Ambient documentation uses AI to passively capture a clinical encounter, including the conversation, vitals, and contextual signals, and produces a structured draft note mapped to the relevant EHR fields. The clinician reviews, edits, and signs the note. The keyboard becomes the exception rather than the default, and clinical judgment remains with the clinician at every step.
Not at all. The Nurse-in-the-Loop model explicitly keeps clinical judgment with the clinician. AI handles capture, synthesis, and drafting; the clinician handles review, contextualization, and final accountability. Every AI-generated output is editable and auditable, and every deployed model is monitored for drift. The objective is to remove drudgery, not delegate decisions.
Capacity programs should be measured on five outcomes: clinician time returned per shift, after-hours EHR work reduced, agency and overtime expense displaced, voluntary turnover trend, and patient-facing quality indicators such as falls, readmissions, and patient experience scores. Throughput-only metrics tend to recreate the burnout the program was meant to solve, so they should never be the lead measure.
